|
|
Anterior Hip Dislocation
General Considerations
- Hip dislocation accounts for only 5% of all dislocations
- Posterior hip dislocations are much more common than anterior hip dislocations (90% to about 10%)
- Mechanism in anterior dislocation classically occurs when knee strikes dashboard with the thigh abducted, externally rotated with hip flexed
- Also falls from a height
- Blow to the back while in squatted position
- Greater force required to dislocate an adult's hip than a child's
Clinical Findings
- Severe pain, inability to move limb and numbness
- Affected limb is sometimes shortened, usually abducted, and externally rotated
- Signs of vascular or sciatic nerve injury
- Pain in hip, buttock, and posterior leg
- Loss of sensation in posterior leg and foot
- Loss of dorsiflexion (peroneal branch) or plantar flexion (tibial branch)
- Loss of deep tendon reflexes (DTRs) at the ankle
- Local hematoma
Imaging findings
- Conventional radiography
- In anterior dislocations, the head of the femur usually rests inferior and medial to its normal acetabular position, frequently overlying the obturator foramen (inferior type of anterior dislocation)
- Some anterior dislocations the femoral head may lie superior to the acetabulum (superior type of anterior dislocation)
- These occur when mechanism is abduction, external rotation, and extension rather than flexion of the leg
- The superior type of anterior dislocation may be confused with a posterior dislocation
- May be subtle if head in AP plane appears as if it still resides in the acetabulum
- There may be associated fractures of the anterosuperior aspect of the femoral head (indentation fracture) or greater trochanter
- Since the anteriorly dislocated head lies farther from the cassette, the anteriorly dislocated head may appear larger than the head on the opposite side which lies closer to the cassette and is magnified less
- Computed tomography (CT)
- Provides an accurate means of evaluating not only the dislocation but the associated fractures as well
Treatment
- Requires immediate pain management
- Reduction of the dislocation within 6-12 hours
- Avascular necrosis (AVN) of the femoral head is more likely to occur if the reduction does not occur before 6 hours
- AVN of the femoral head occurs in 10% of anterior hip dislocations
Prognosis
- Good-to-excellent results in most patients

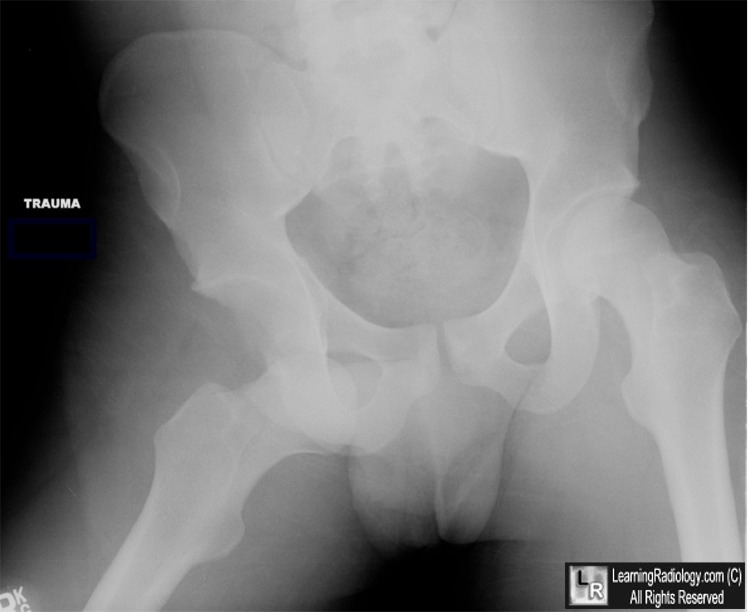
Anterior Hip Dislocation. The right femoral head (blue arrow) overlies the obturator foramen,
inferior and medial to its normal location in the acetabulum (white arrow).
For this same photo without the arrows, click here
For more information, click on the link if you see this icon 
Posterior Hip Dislocations. Emedicine. J Naradzay, MD and P Carter, MD
Wheeless Online Textbook of Orthopedics
|
|
|

{kind=link}